GMLOS vs. ALOS
Many important metrics characterize the multifaceted world of healthcare, each profoundly impacting health services’ operational, financial, and clinical facets. One such critical indicator is the measurement of the hospital stay duration, commonly referred to as the average length of stay (ALOS). It is used extensively in healthcare management as it paints a detailed panorama of patient flow, the efficiency of care processes, the hospital’s economic health, and a reflection of the quality of care provided to the patients.
Another essential hospital measurement is the Geometric Mean Length of Stay (GMLOS), which attempts to respond to skewed healthcare data where outliers can distort an accurate reflection of patient experiences. Both GMLOS and ALOS are intimately interlinked; however, their calculation methodologies offer subtly different insights into healthcare management.
The ALOS can be defined as the mean length of a hospital stay. It is calculated using the Average Length of Stay Formula. This formula adds up the total length of hospital stay of all admissions within a given period and divides it by the total number of admissions during the same period. This metric provides key insights into resource utilization and the effectiveness of treatment processes that influence policy-making.
Conversely, the definition of GMLOS revolves around the average length of inpatient stays, adjusted for patients’ severity of illness. This includes severity adjustments for the complexity of cases, allowing for a more accurate comparison across different hospitals. GMLOS in the medical field is observed through Diagnosis Related Groups (DRGs), which assign patients with similar clinical conditions and resource use to the same group.
The DRG-based GMLOS is essential to both clinical and financial decision-making. Understanding both ALOS and GMLOS assists in comprehensively evaluating factors such as medical care quality, operational efficiency, patient flow, and hospital resource usage against the backdrop of healthcare decision-making. Undeniably, these metrics are not merely numbers but significant indicators driving healthcare accessibility, affordability, and care delivery.
Hence, the main topic of GMLOS vs. ALOS forms a central component in the narrative of efficient hospital management and information that is crucial for both healthcare professionals and the general public.
Understanding ALOS
The world of healthcare is fraught with myriad terminologies and metrics that can sometimes be disconcerting to those not accustomed to healthcare management. Among these various measures, the average length of stay (ALOS) is a pivotal factor in understanding healthcare efficiencies.
In simple terms, ALOS refers to the average number of days that patients spend in a hospital. This is calculated by dividing the total number of days stayed by all inpatients during a period by the number of admissions or discharges during the same period. To delve deeper into the calculation of ALOS, let’s break down the formula. ALOS is computed by dividing the total inpatient days (or bed days) by the total number of discharges, including deaths, in a specified period.
For instance, if a hospital had 300 bed days and 100 discharges in a month, the ALOS would be three days. It’s a relatively straightforward calculation that provides a measure of the efficiency of hospital services. ALOS plays a significant role in healthcare management. It serves an indispensable function in gauging the efficacy of hospital management, enabling healthcare providers to assess the healthcare facility’s utilization efficiency.
Understanding ALOS assists in managing resources effectively, checking cost-effectiveness, and aiding hospitals in estimating future bed availability. Furthermore, it also allows healthcare facilities to identify performance issues and determine areas that may benefit from process improvements.
Nevertheless, depending entirely on ALOS as a measure of efficacy can lead to potential pitfalls. Essentially, ALOS is an average, meaning it doesn’t account for the variability or the distribution of stay lengths.
Therefore, it might not effectively reflect individual patient experiences. For instance, a single extraordinarily long or short stay can skew the average, thereby underrepresenting the typical patient experience. Despite these shortcomings, ALOS remains a meaningful measure in the arsenal of healthcare efficiency indicators.
Ultimately, understanding the nuances of ALOS, its calculation, and its implications in healthcare allows hospitals to deliver better, more efficient care. By providing an example of an average length of stay, we can illustrate how healthcare facilities use this measure to gauge their efficiency and identify areas for improvement. Despite potential disadvantages, ALOS remains an essential tool for healthcare management analysis, reflecting its fundamental role in healthcare efficiency.
Digging Deeper Into GMLOS
The realm of healthcare management is full of acronyms and measures that are often tricky to decipher for those tied at the periphery. Yet, amidst this muddy field of abbreviations and numerical values, the term GMLOS stands prominent as a multipurpose metric, reflecting the overall efficiency of a healthcare facility.
Derived from a complex mix of patient-level data, it is calculated by taking the geometric mean of the patient’s length of stay. As the term geometric hints, it is a more complex arithmetic mean. The GMLOS attaches more weightage to shorter-stay cases rather than long-stay cases, providing a more centered value apt to summarize a wide range of data.
Therefore, GMLOS provides a measure that is more balanced and realistic. In essence, the GMLOS represents an average length of stay that heavily factors patient acuity, hospital resource utilization, and quality of care. By comparing it with ALOS, we get a clearer view of its advantages. Unlike ALOS, GMLOS addresses outliers and skewed data, providing a more robust measure for managerial decisions and provider comparisons.
However, GMLOS must be case-mixed adjusted for fair comparisons. Designed for this purpose are the CMS GMLOS and the DRG GMLOS. Providing case-mix adjustment, these measures allow more accurate comparisons across facilities with differing patient demographics and disease severity. As much as it is sophisticated, the power of GMLOS lies in the depth of its interpretation.
This is where the term GMLOS O/E comes into play. Representing “Observed over Expected,” it acts as an essential scale for judging the performance of a healthcare facility against industry-standard benchmarks.
However, deriving all these from a GMLOS calculator is an intricate task. This numerical tool requires comprehensive data from numerous patient encounters, expert data analysis, and an understanding of the GMLOS formula.
Therein lies the limitation. It requires in-depth expertise and resources, often needing improvement for many healthcare facilities. But despite the complexities, these measures are vital in optimizing healthcare resource use and, ultimately, patient outcomes for the benefit of all stakeholders in this dynamic field.
The Connection Between CMS, GMLOS, and DRGS
The world of healthcare language can be confusing, with a myriad of acronyms like CMS, GMLOS, and DRGs intertwined in a technical discourse. However, demystifying these terms can unlock an extensive understanding of the healthcare system’s structure, particularly in terms of provider payment mechanisms and patient care cost deciphering.
The power player in this convoluted network is the CMS (the Centers for Medicare and Medicaid Services). CMS is the federal agency responsible for administering national healthcare programs and defining crucial parameters, such as the GMLOS or Geometric Mean Length of Stay, a significant factor in determining provider reimbursements under Medicare.
In essence, GMLOS predetermines the average length of time a patient will stay in the hospital for a particular diagnosis or procedure. The connection between CMS, GMLOS, and DRGs (Diagnosis-Related Groups) succinctly portrays this reimbursement mechanism. In particular, DRGs are a cornerstone concept in the CMS framework. DRGs are used in a prospective payment system (PPS) where hospitals are compensated a fixed amount for each patient stay, determined by the DRG code assigned to that case.
This makes DRG codes much like a language of economics in healthcare. Thus, a list of DRG codes and descriptions can be informative, providing invaluable insights into the expected patient care costs. The correlation between GMLOS and DRGs is integral to calculating the CMS length of stay. Each DRG is allocated a specific GMLOS, calculated based on historical patient data, reflecting the average hospital stay for patients within that DRG. This impacts CMS DRG reimbursements because shorter stays that fall below the GMLOS can yield higher margins for providers, whereas more extended stays can potentially lead to less revenue.
Therefore, understanding these parameters and their interconnected dynamics is pivotal for successful healthcare management. While the rapport amongst CMS, GMLOS, and DRGs can appear intricate, uncovering and decoding this connection lends crucial insights into healthcare cost management.
By comprehending how measures like GMLOS are intertwined with DRG code allocation and CMS regulations, healthcare professionals can effectively navigate the complexities of healthcare economics. The endeavor improves financial management efficiencies and contributes towards optimizing patient care delivery strategies.
GMLOS vs ALOS: A Comparative Analysis
GMLOS and ALOS – the geometric mean length of stay and the arithmetic mean length of stay, respectively – are handy metrics in healthcare management and analysis. Whether you’re an analyst seeking to streamline services or a healthcare provider striving to optimize patient care, these two measurements can provide insightful information. In better understanding these terms, let’s first focus on GMLOS or the geometric mean length of stay.
This method involves a calculation of a geometric length of stay that offers a highly accurate mean. Far from a simple average, the GMLOS considers the entire distribution of lengths of stay, thus accounting for the long or short stays that could disproportionately sway an arithmetic mean.
On the other hand, we encounter ALOS, the arithmetic mean length of stay. Arguably a simpler concept, ALOS merely necessitates dividing the sum of inpatient days by the number of inpatients. This uncomplicated calculation offers a straightforward, if somewhat broad, picture of a patient’s stay duration. But make no mistake about its importance: ALOS is pivotal to managing and planning resources like staffing and supply needs effectively. While both GMLOS and ALOS are valuable in their own right, each serves specific purposes and offers distinct benefits.
For instance, the GMLOS, when compared to ALOS, can provide a more accurate picture of the length of stay, especially when there may be significant variations. By offering a more nuanced perspective, GMLOS may assist institutions in identifying areas of inefficiency, thus paving the way for meaningful improvements.
Meanwhile, ALOS gives an overarching view, which can assist organizations in understanding their usual patient stay length. This data can be invaluable for resource allocation, staff scheduling, etc. To further illustrate these concepts, consider a real-world scenario.
Suppose a hospital strives to reduce the length of stay for a specific procedure. In this case, both GMLOS and ALOS can play into the analysis. The GMLOS could reveal the typical length of stay or the goal length of stay, while the ALOS might show the range of stay lengths. Armed with this information, this hospital could strategize more effectively to achieve its goal.
A calculated approach involving both AMLOS vs GMLOS ensures healthcare organizations reap the full benefits of each approach and navigate the complexities of the healthcare landscape with sophistication and agility. By juxtaposing these two methods, we can appreciate the rich tapestry they weave, playing indispensable roles in shaping healthcare outcomes and experiences.
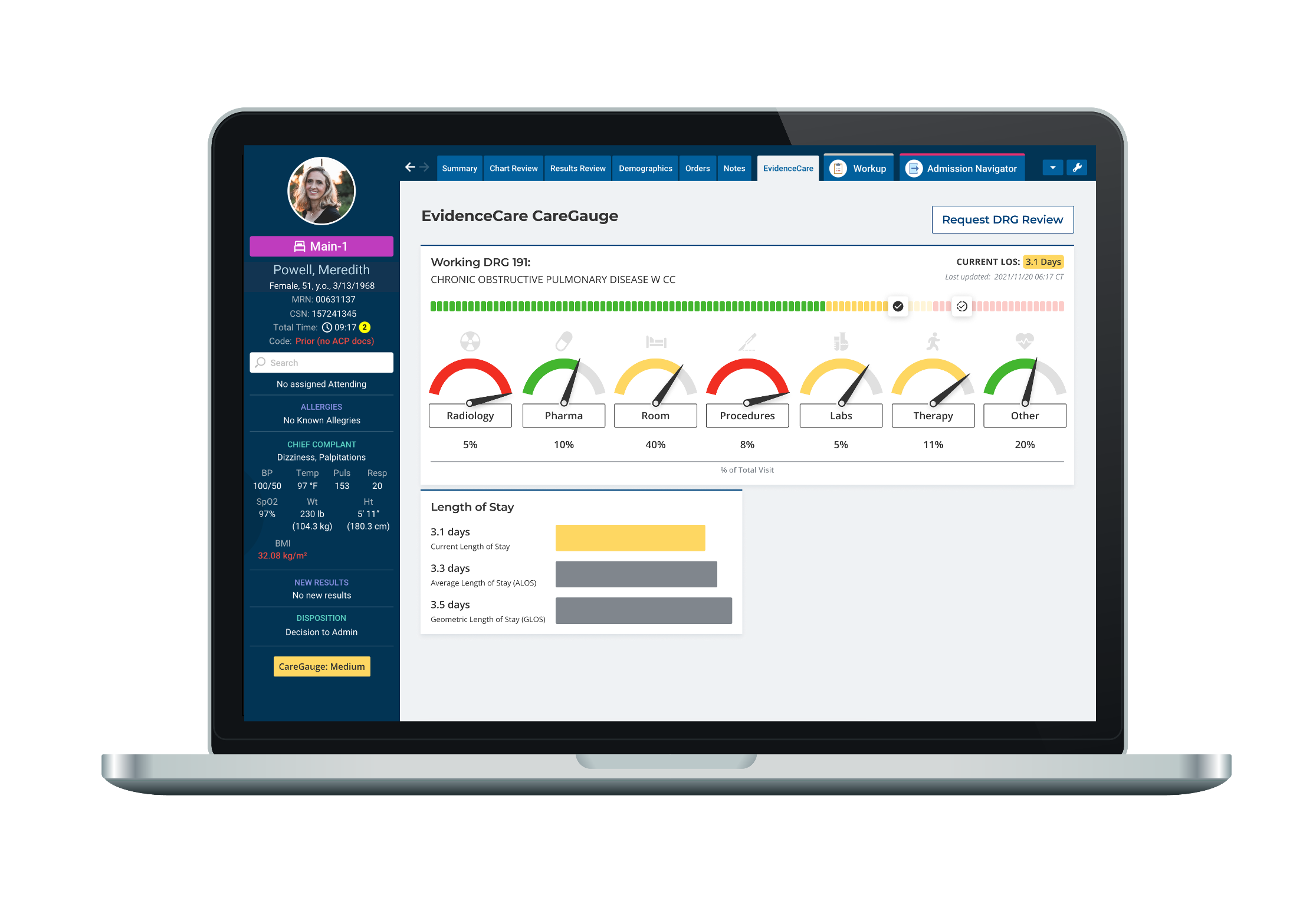
EvidenceCare’s software, CareGauge, uses automated DRG calculations to give physicians average length of stay insights at the point of care, in their EHR workflow. This makes it easier to adjust care plans in real-time instead of looking at retrospective length of stay reports. To learn more, schedule a demo of CareGauge today.